Fast Facts
- Gay, bisexual, and other men who have sex with men (referred to here as MSM) are more severely affected by HIV than any other group in the United States.
- Among all MSM, black/African American MSM bear the greatest disproportionate burden of HIV.
- From 2008 to 2010, HIV infections among young black/African American MSM increased 20%.

Gay, bisexual, and other men who have sex with men (MSM))a
represent approximately 2% of the United States population, yet are the
population most severely affected by HIV.
In 2010, young MSM (aged
13-24 years) accounted for 72% of new HIV infections among all persons
aged 13 to 24, and 30% of new infections among all MSM.
At the end of
2010, an estimated 489,121 (56%) persons living with an HIV diagnosis in
the United States were MSM or MSM-IDU.
The Numbers
New HIV Infectionsb
- In 2010, MSM accounted for 63% of estimated new HIV infections in the United States and 78% of infections among all newly infected men. From 2008 to 2010, new HIV infections increased 22% among young (aged 13-24) MSM and 12% among MSM overall.
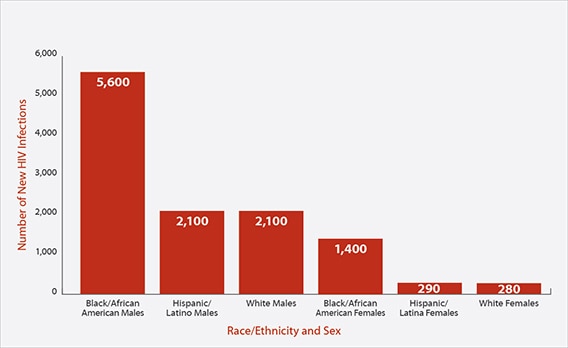
- Among all MSM, white MSM accounted for 11,400 (38%) estimated new HIV infections in 2010. The largest number of new infections among white MSM (3,300; 29%) occurred in those aged 25 to 34.
- Among all MSM, black/African American MSM accounted for 10,600 (36%) estimated new HIV infections in 2010. The largest number of new infections among black/African American MSM (4,800; 45%) occurred in those aged 13 to 24. From 2008 to 2010 new infections increased 20% among young black/African American MSM aged 13 to 24.
- Among all MSM, Hispanic/Latino MSM accounted for 6,700 (22%) estimated new HIV infections in 2010. The largest number of new infections among Hispanic/Latino MSM (3,300; 39%) occurred in those aged 25 to 34.
Estimates of New HIV Infections in the United States for the Most-Affected Subpopulations, 2010

Source: CDC.
HIV Surveillance Supplemental Report 2012;17(4).
Subpopulations representing 2% or less of the overall US epidemic are
not reflected in this chart. Abbreviations:
MSM, men who have sex
with men; IDU, injection drug user.
HIV and AIDS Diagnosesc and Deaths
- In 2011, in the United States, MSM accounted for 79% of 38,825 estimated HIV diagnoses among all males aged 13 years and older and 62% of 49,273 estimated diagnoses among all persons receiving an HIV diagnosis that year.
- At the end of 2010, of the estimated 872,990 persons living with an HIV diagnosis, 440,408 (50%) were MSM. Forty-seven percent of MSM living with an HIV diagnosis were white, 31% were black/African American, and 19% were Hispanic/Latino.
- In 2011, MSM accounted for 52% of estimated AIDS diagnoses among all adults and adolescents in the United States. Of the estimated 16,694 AIDS diagnoses among MSM, 39% were in blacks/African Americans; 34% were in whites; and 23% were in Hispanics/Latinos.
- By the end of 2010, an estimated 302,148 MSM with an AIDS diagnosis had died in the United States since the beginning of the epidemic, representing 48% of all deaths of persons with an AIDS diagnosis.
Prevention Challenges
The large number of MSM living with HIV means
that, as a group, gay, bisexual, and other MSM have an increased
chance of being exposed to HIV.
Results of HIV testing conducted in 20
cities as part of the National HIV Behavioral Surveillance System
indicated that 18% of MSM tested in 2011 were HIV-positive and that HIV
prevalence increased with increasing age.
In this study, the overall percent of gay and
bisexual men with HIV who knew of their HIV infection increased from
56% in 2008 to 66% in 2011.
Among those infected, 49% of young MSM aged
18 to 24 years knew of their infection, whereas 76% of those aged 40
and over were aware of their HIV infection.
Fifty- four percent of
black/African American MSM knew of their infection, compared with 63%
of Hispanic/Latino MSM and 86% of white MSM.
Persons who don’t know
they have HIV don’t get medical care and can unknowingly infect others.
The Centers for Disease Control and Prevention (CDC) recommends that
all MSM get tested for HIV at least once a year. Sexually active MSM
might benefit from more frequent testing (e.g., every 3 to 6 months).
Sexual risk behaviors account
for most HIV infections in MSM. Anal sex without a condom (unprotected
anal sex) has the highest risk for passing HIV during sex.
It is also
possible to become infected with HIV through oral sex, though the risk
is significantly less than for anal or vaginal sex.
For sexually active
MSM, the most effective ways to prevent HIV are to limit or avoid anal
sex, or for MSM who do have anal sex, to correctly use a condom every
time.
Gay men are at increased risk for sexually transmitted infections
(STIs), like syphilis, gonorrhea, and chlamydia, and CDC recommends
that all sexually active MSM be tested annually for these infections.
Alcohol and illegal drug use increases
risk for HIV and other STIs. Using substances such as alcohol and
methamphetamines can impair judgment and increase risky sexual
behavior.
Homophobia, stigma, and discrimination may place
gay men at risk for multiple physical and mental health problems and
affect whether they seek and are able to obtain high-quality health
services.
What CDC Is Doing
Guided by the National HIV/AIDS Strategy for the United States, CDC and its partners are pursuing a
high-impact prevention approach to reducing new HIV infections by using
combinations of scientifically proven, cost-effective, and scalable
interventions directed to the most vulnerable populations in the
geographic areas where HIV prevalence is highest.
for the United States, CDC and its partners are pursuing a
high-impact prevention approach to reducing new HIV infections by using
combinations of scientifically proven, cost-effective, and scalable
interventions directed to the most vulnerable populations in the
geographic areas where HIV prevalence is highest.
As part of high-impact prevention, CDC is aligning surveillance and program activities more closely.
For example, while linkage to care soon after HIV diagnosis is
relatively high, more people living with HIV should receive continuous
care and antiretroviral treatment, and a greater proportion of persons
infected with HIV should have a suppressed HIV viral load—the most
important goal for maximizing a person’s health as well as reducing the
risk of transmission.
By increasing the reporting of CD4 and viral
load data across the country, CDC will aid health departments and
clinicians in monitoring treatment progress toward viral load
suppression. Currently, CDC estimates that only 25% of the 1.1 million
individuals with HIV have their viral loads adequately suppressed.
CDC is also encouraging MSM and their healthcare providers to take advantage of biomedical approaches to HIV prevention.
Pre-exposure prophylaxis (PrEP),
which involves taking antiretroviral medications prior to becoming
exposed to HIV, can reduce the risk of HIV infection in individuals at
very high risk of infection.
Post-exposure prophylaxis,
which involves taking antiretrovial medications soon after possible
exposure to HIV, also plays a role in HIV prevention, but should be not
be considered a primary means of HIV prevention.
Also, while HIV
treatments can dramatically improve the health of HIV-positive persons
who are treated, they also have prevention benefits: individuals whose
HIV viral loads are suppressed have a greatly reduced chance of
transmitting the virus to their partners (Treatment as Prevention).
CDC continues to focus on HIV testing.
To expand HIV prevention services for young gay and bisexual men of
color, transgender youth of color, and their partners, CDC awarded $55
million over 5 years to 34 community-based organizations with strong
links to these populations.
This funding will be used to provide HIV
testing to more than 90,000 young gay and bisexual men and transgender
youth of color, with a goal of identifying more than 3,500 previously
unrecognized HIV infections and linking those who are HIV-infected to
care and prevention services.
Additionally, CDC’s MSM Testing
Initiative seeks to identify at least 3,000 MSM with HIV who were
previously unaware of their infection and link at least 85% to care.
Through its Act Against AIDS
campaigns and other collaborative activities, CDC aims to provide MSM
with effective and culturally appropriate messages about HIV
prevention.
The REASONS/RAZONES testing campaign features Latino gay and bisexual men sharing their reasons for getting an HIV test, while Testing Makes Us Stronger campaign encourages black gay and bisexual men to get tested for HIV.
Let’s Stop HIV Together focuses
on raising awareness of HIV and AIDS and simultaneously combatting
complacency and stigma by increasing support for people living with the
disease.
CDC also funds state and local health departments and community-based organizations to support HIV prevention services for MSM. Through the Diffusion of Effective Behavioral Interventions (DEBI) project, CDC supports various behavioral interventions and other high-impact prevention strategies.
CDC also funds state and local health departments and community-based organizations to support HIV prevention services for MSM. Through the Diffusion of Effective Behavioral Interventions (DEBI) project, CDC supports various behavioral interventions and other high-impact prevention strategies.
Read more about CDC activities to reduce HIV risk and improve the health of MSM.
For more background information view the bibliography and other references used in this factsheet.
a The term men who have sex with
men (MSM) is used in CDC surveillance systems.
It indicates the
behaviors that transmit HIV infection, rather than how individuals
self-identify in terms of their sexuality.
b New HIV infections refer to HIV incidence, or the estimated number of people who are newly infected with HIV each year.
c HIV and AIDS diagnoses are the number of persons diagnosed with HIV infection and the number of persons diagnosed with AIDS, respectively, during a given time period.
The
terms do not indicate when the persons were infected.